 Join our
Join our
Health Bulletin - April 2023
The Heart of the Matter: South Asian Women and Heart Disease
More women die from heart disease than any other cause. This article will discuss myths about heart disease, how heart disease affects women differently, and what women can do to take control of their heart health.
Heart disease is truly an “equal-opportunity illness” and is the number one killer of women just as in men. Heart disease kills more women than all forms of cancer combined and approximately 6 times more than breast cancer, according to the American Heart Association. And unfortunately, only about half of women are aware of this fact. Additionally, being of South Asian origin confers significant risk for heart disease. Heart disease is considered a silent epidemic among Indians and people of Indian origin. Heart disease strikes Indians at an earlier age; usually a decade younger compared to other ethnicities.
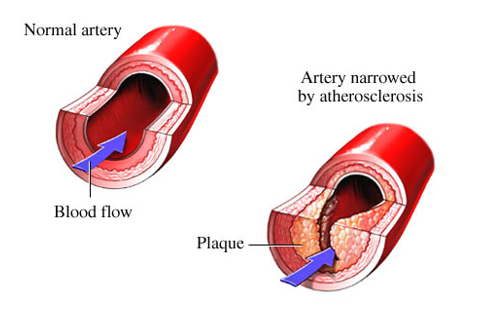
The heart is the most hard-working muscle of our body pumping approximately 4-5 liters of blood every minute supplying nutrients and oxygen rich blood to all body parts, including itself. The blood vessels supplying the heart muscle are called coronary arteries. Over time, fatty deposits called “plaque” build up within the walls of these coronary arteries, a process called atherosclerosis. This leads to narrowing of the lumen and thereby compromising the blood flow to the heart muscle, also known as coronary artery disease.
Risk factors for coronary artery disease: There are non-modifiable risk factors like age, gender, post-menopausal state for women, ethnicity, and family history. The traditional risk factors, most of which we can modify, include diabetes (elevated blood glucose levels), hypertension (high blood pressure), hyperlipidemia (elevated cholesterol levels), obesity, smoking, lack of physical activity, and chronic kidney disease. Having said that, eighty percent of overall health is shaped by non-clinical factors in the social, economic, and physical environments we live in including chronic stress.
Diabetes: Diabetes is a chronic health condition related to increased blood sugar levels. Indian men and women are particularly prone to diabetes due to genetic predisposition; six times more than our Caucasians. A carbohydrate rich diet with increasing fast-food consumption added to our inherent genetic risk leads to the perfect storm. Diabetes is bad for men but worse for women. Diabetic women are more likely to die from heart problems compared to diabetic men. Symptoms of diabetes include tiredness, weight gain, excess appetite, increased thirst, increased need to urinate and vision changes. Diabetes enhances the plaque building process of atherosclerosis and hence early detection and aggressive treatment and lifestyle changes are necessary to maintain heart health.
Hypertension: High blood pressure is associated with age and our risk of heart disease doubles with a 20-point increase in systolic blood pressure (upper number). Approximately every third adult south asian has a diagnosis of high blood pressure. For women specifically, pregnancy related high blood pressure confers a markedly increased risk for developing early onset heart disease. Awareness and early detection with treatment of high blood pressure can prevent heart disease.
Hyperlipidemia: There are two primary sources of cholesterol, cholesterol that is made by our body and cholesterol that we consume from foods like animal fats and meat products.
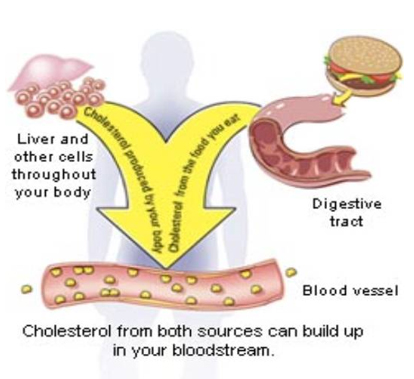
LDL cholesterol is bad because it leads to the plaque buildup within the walls of our blood vessels there by increasing the risk for heart attacks. On the other hand, the HDL cholesterol is good as it carries the bad cholesterol from other parts of the body to the liver which then helps remove the bad cholesterol from the blood. Triglycerides is another type of fat component that increases heart disease risk. For any given cholesterol level, the risk of heart disease is double for south asians compared to that of other ethnic groups. Hence, the goal level of total and LDL cholesterol is lower for our community.
Smoking: Smoking hurts women more than men and female smokers are 25% more likely to develop coronary artery disease than male smokers.
Metabolic Syndrome: The combination of excess abdominal fat, high blood pressure, high blood sugar and high triglycerides is a particularly strong predictor for heart disease in south Asian women. Women under the age of 45 with metabolic syndrome are at risk for premature coronary artery disease.
Postmenopausal state: Natural Estrogen, the female hormone, is protective towards heart health. Estrogen lowers inflammation, a key process involved in plaque buildup in our blood vessels. Estrogen helps lower bad cholesterol (LDL) and triglycerides and helps in increasing good cholesterol (HDL). Additionally, Estrogen helps lower the BP and lower the free radicals which are particles that can cause damage to human cells and contribute to aging. When estrogen levels start to decline at menopause, the risk for heart disease not only increases but surpasses that of a man with similar age and risk profile. Hormone replacement therapy (HRT) commonly used to relieve post-menopausal symptoms did not turn out to be beneficial in mitigating the heart disease risk. A large, randomized study done on this subject revealed a small increase in heart disease and significant risk of blood clots with HRT. If you are considering HRT for your post-menopausal symptoms, you should first have a thorough evaluation of risk for heart disease.
Non-traditional risk factors: Women with recurrent miscarriages and systemic inflammatory diseases like Lupus and Rheumatoid Arthritis are at very high risk for developing heart disease earlier. Additional factors like elevated lipoprotein (a) and C-reactive protein, which is a measure of inflammation in the body are also considered important for heart disease risk in south asian women.
Symptoms of Heart disease in women: The most common heart attack symptom in women is the same as in men, some type of chest pain, pressure or discomfort that lasts more than a few minutes or comes and goes. However, chest pain is not always severe or even the most noticeable symptom, particularly in women. Women are more likely than men to have heart attack symptoms unrelated to chest pain, such as discomfort in neck, jaw, shoulder, upper back or upper belly, shortness of breath, pain in one or both arms, nausea or vomiting, sweating, lightheadedness or dizziness, unusual fatigue, and heartburn (indigestion). If you have any mix of these symptoms, please call 911. Do not drive yourself to the emergency department unless you have no other option.
Ways to prevent heart disease: Being aware of your health status and your family history is a great place to start with. Make sure you are providing your body with regular physical activity (30 minutes of brisk walking at least 5 days a week) and proper nutrition which includes a wide variety of fruits and vegetables, whole grains, healthy sources of protein (mostly plant based such as legumes and nuts; fish and seafood; low-fat or nonfat dairy products and, if you eat meat and poultry, ensuring it is lean and unprocessed), plant based cooking oils like Canola, corn, olive, peanut, safflower, sesame, soybean and sunflower oils, lower intake of added sugars and lower the salt content, limited or preferably no alcohol intake. Embrace relaxation and stress reduction strategies with yoga, music, meditation or spending time on a favorite hobby.
See your doctor for regular preventative care. The rule of thumb is to go to the doctor 10 years before your parent had their first heart-related incident. If you have a family history and father had heart condition younger than 50 and mother younger than 55, start seeking help 10 years before. Your primary care doctor can start assessing your risk profile with lab work, calculate your heart disease and stroke risk scores and in some cases request a study called coronary calcium scoring test which gives an estimate of calcified plaque that is already built up in your blood vessels supplying your heart. High cholesterol can run in families and in such cases, diet alone cannot make a difference and medicines are needed to maintain an optimal level of cholesterol. If you have no family history, anybody at the age of 40 should have annual checkup with yearly blood pressure check, glucose level/hemoglobin a1c and cholesterol panels.
Put the Oxygen mask on yourself first: We have heard this multiple times during our flight journeys, but this statement truly reflects women and their health. “I thought it couldn’t be true. In my mind, I take care of other people. There’s no way that I will be the one who has to be cared for.” These are the words from a woman who survived a massive heart attack. Remember that your commitment to your family cannot be met unless you make a commitment to yourself first. By putting care off, you are risking your own health along with your ability to care for your loved ones. Take a moment from your busy lives and start caring for your heart.

Meera Kondapaneni, MD, FACC, FSCAI
Associate Professor of Medicine, Case Western Reserve University School of Medicine
Director, Heart and Vascular Center, MetroHealth Medical Center
Article Coordinated by
Dr. Sujeeth R. Punnam, MD
Chair, Health Committee
(Dr. Sujeeth R. Punnam is a cardiologist in Stockton, California and is affiliated with Dameron Hospital and St. Joseph's Medical Center. He received his medical degree from Kakatiya Medical College and has been in practice for more than 20 years.)






































